Interpretation of Physical Signs
Physical examination is an art. It should be goal-oriented with the aim of gathering relevant clinical information to help diagnose the underlying cardiac condition. Physical signs gathered, whether normal (so-called 'negative' signs ) or abnormal (so-called 'positive' signs), would help to support a particular diagnosis and/or exclude differential diagnoses. Describing the signs as being 'negative' or 'positive' is therefore not entirely appropriate. Auscultation alone is not cardiovascular examination. One should refrain from making a cardiac diagnosis based on auscultatory findings alone. The signs gathered from general inspection, pulse examination, praecordial inspection and palpation, auscultation, and examination of other relevant systems need to be interpreted in a holistic fashion to arrive at a diagnosis or a short list of differential diagnoses.
Failure to thrive Physical growth parameters should be measured and plotted onto standard growth chart for serial monitoring of the changes in growth percentiles. The presence of failure to thrive in infants with heart disease usually signifies the presence of large left-to-right shunts. In these infants, the weight percentile usually drops before the drop in height percentile and head circumference. With uncontrolled heart failure, the height percentile will also fall, although the head circumference is usually spared.
Dysmorphism New genomic techniques have made significant advances in the understanding of copy number variants, syndromes, and RASopathies in the pathogenesis of congenital heart disease. Associations between dysmorphic features and congenital heart disease are well documented in genetics disorders and syndromes (see section on Guidelines and Reviews).
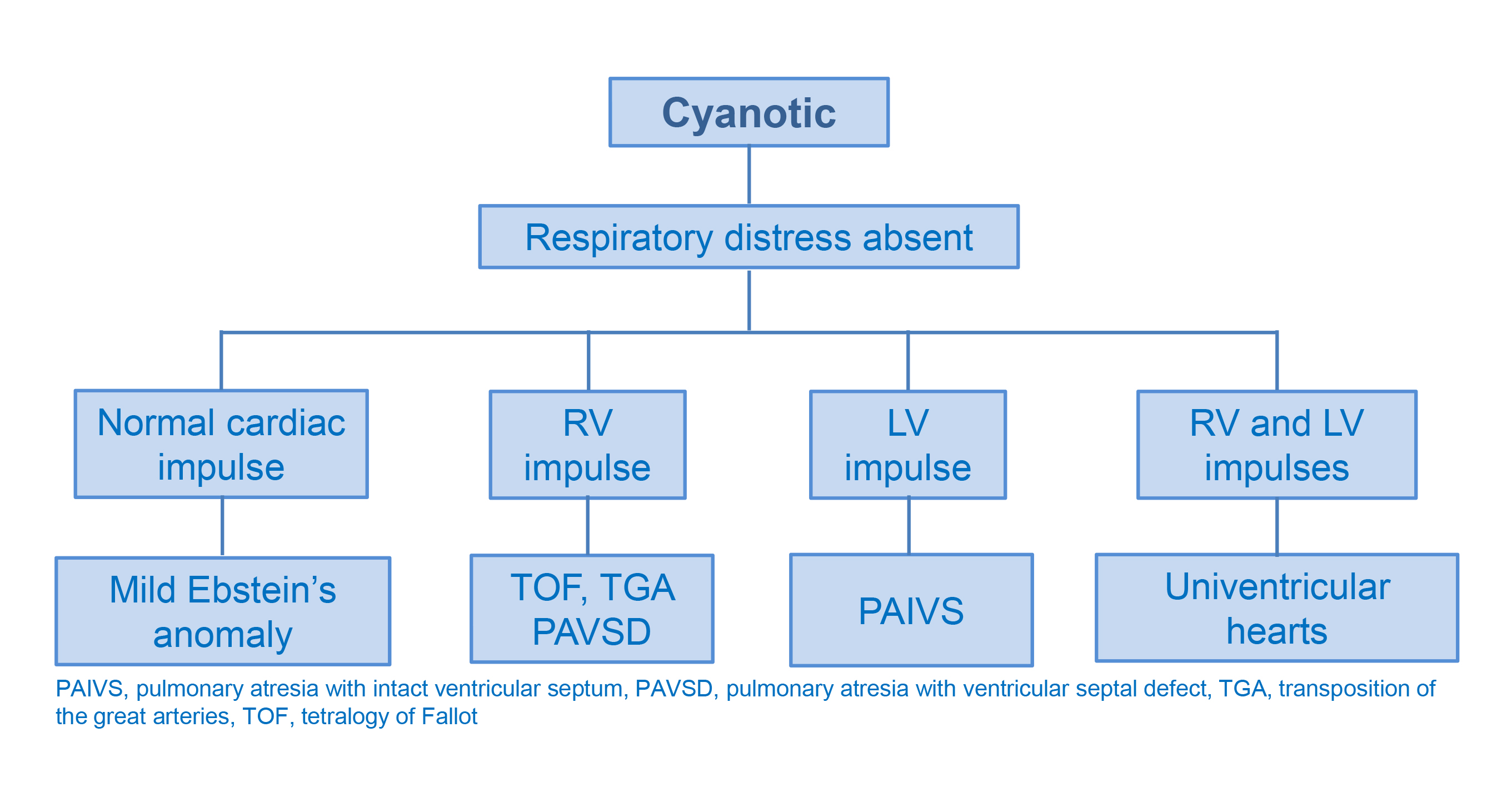
Cyanosis Cyanosis Central cyanosis occurring in the absence of respiratory distress usually signifies an underlying cyanotic heart condition. On the other hand, the presence of respiratory distress suggests possible parenchymal disease of the lungs and airway disorders as the cause of cyanosis. Cyanosis can, however, be masked by severe anaemia. The presence of anaemia may confound the clinical assessment Severity of cyanosis is ...
Clubbing Chronic cyanosis is associated with finger and toe clubbing. In patients with chronic hypoxaemia due to cyanotic congenital heart disease, the finger and toe clubbing may persist even after complete surgical repair. Hence, the presence of clubbing and a mid-sternotomy scar in an otherwise acyanotic child suggests cyanotic heart disease post repair.
Arachnodactyly In a child with tall stature and long and slender fingers, one should examine other features suggestive of Marfan syndrome. The following additional clinical signs should be sought: wrist sign, thumb sign, joint laxity, pectus abnormalities, pes planus, scoliosis, reduced upper segment to lower segment ratio and increased arm span/height, and skin striae. Diagnosis of Marfan syndrome is based on the revised Ghent nosology.
Wrist sign The wrist sign is positive when the top of the thumb covers the entire fingernail of the fifth finger when wrapped around the wrist on the opposite side
Thumb sign Thumb sign The thumb sign is positive when the distal phalanx of the thumb protrudes entirely beyond the ulnar border of a clenched fist with maximum thumb adduction.
Edema Peripheral edema occurs in congestive heart failure as a result of the two factors: i) neurohumoral activation with promotion of sodium and water reabsorption, and ii) abnormal Starling forces due to increased venous capillary pressure and/or decreased plasma oncotic pressure. As Starling forces are usually normal in infants with heart failure due to left-to-right shunts, peripheral edema is distinctly uncommon. On the other hand, in children and adolescents with cardiomyopathies, both factors work in concert to cause ankle edema.
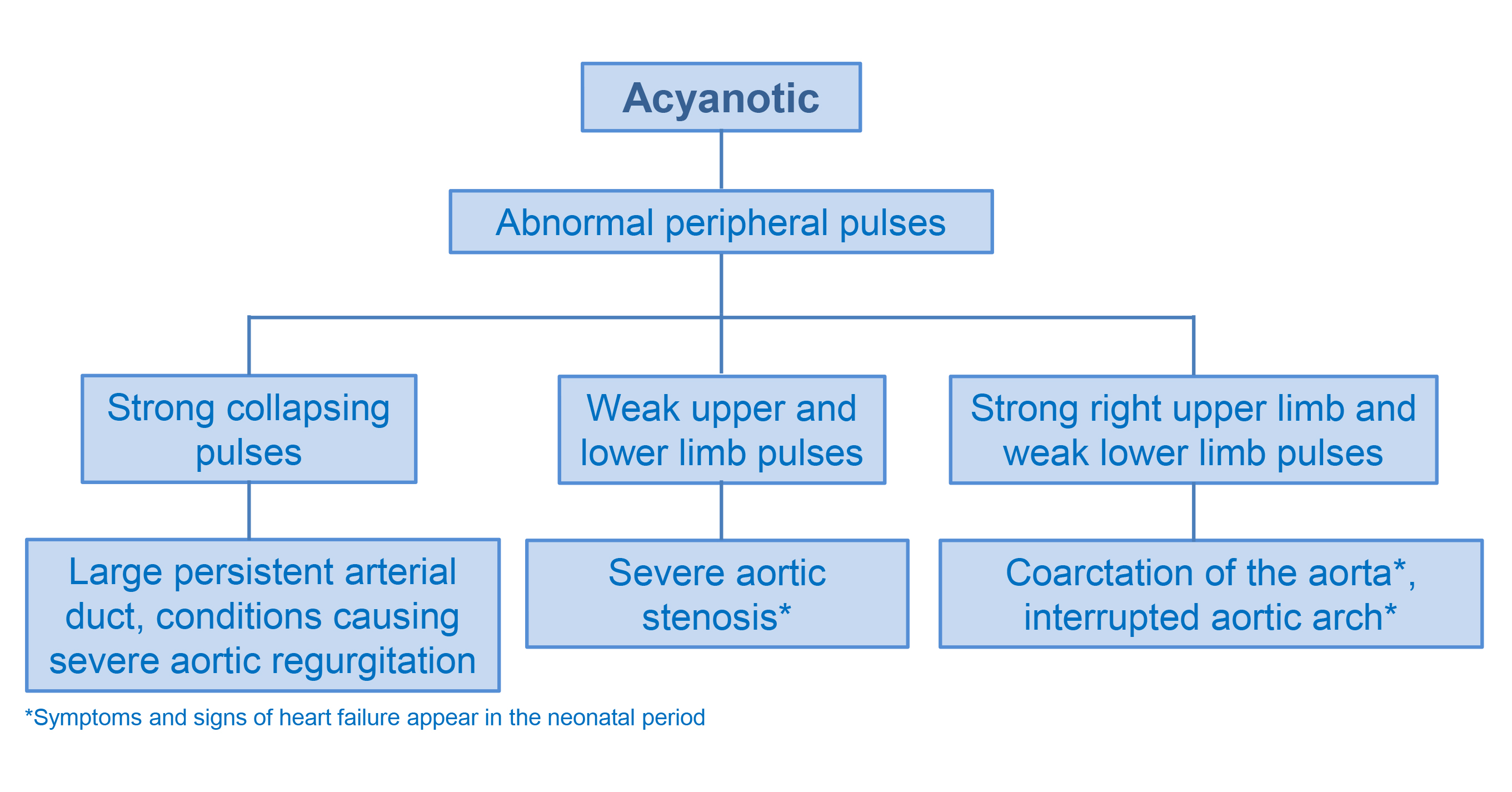
Increased arterial pulsation In the presence of a large persistent arterial duct or severe aortic regurgitation, the pulse volume is increased. The bounding character reflects a wide pulse pressure caused by a large volume of blood being rapidly ejected from the left ventricle, a low diastolic pressure due to increased diastolic runoff (into the pulmonary arterial circulation or the left ventricle, respectively). The bounding nature may be exaggerated by elevation of the patient's forearm as one feels the radial artery with the distal palmer surface of the hand. A 'collapsing' pulse, as characterized by rapid upstroke and descent of the pulse wave, may be felt.
Diminished arterial pulsation If all of the peripheral pulses are weak, one should consider the possibility of severe aortic stenosis or other causes of low cardiac output syndrome. In severe aortic stenosis, the arterial pulse is slow-rising. If only the femoral pulses are weak or absent, while the upper limb pulses remain strong, one needs to consider the diagnosis of coarctation of the aorta. One should focus on discrepancy between upper and lower limb pulse volumes, as the short aorta in small children may render the detection of radio-femoral pulse delay difficult.
Pulsus paradoxus This term is used to describe the marked fall in systemic arterial pressure during inspiration (>10 mmHg in systolic blood pressure during inspiration in adults). The inspiratory fall in blood pressure is not really paradoxical, but rather exaggerated in conditions including pericardial tamponade, constrictive pericarditis and severe asthmatic attack.
Respiratory distress In children with heart disease, respiratory distress can be due to i) pulmonary arterial congestion as a result of increased pulmonary blood flow (large left-to-right shunts), ii) pulmonary venous congestion due to reduced left ventricular compliance (volume overloading of left ventricle due to large left-to-right shunts, left ventricular systolic dysfunction in dilated cardiomyopathy, left ventricular diastolic dysfunction in restrictive cardiomyopathy), or iii) pulmonary venous or left ventricular inflow (mitral stenosis) obstruction.
Harrison sulcus This groove is seen at the lower part of the rib cage where the diaphragm is inserted in infants and children with chronic respiratory distress. Hence, it can be found in young patients with cardiac conditions, especially large left-to-right shunts, that cause pulmonary vascular congestion and asthma.
Praecordial bulging Bulging of the praecordium is seen in infants and children with cardiomegaly, related usually to large left-to-right shunts. The bulging is most prominent when the right ventricle is dilated, which is usually related to a large atrial septal defect.
Praecordial pulsation Praecordial pulsation Visible cardiac pulsation at the left lower sternal border can be due to volume loading of the right ventricle, commonly due to an atrial septal defect, or pressure loading of the right ventricle, as in severe pulmonary valvar stenosis.
Pectus excavatum Pectus excavatum can be associated with connective tissue disorders including Marfan syndrome, Ehlers-Danlos syndrome, and Loeys-Dietz syndrome. The cardiac associations of these syndromes include enlargement of the aortic root and mitral valve prolapse.
Mid-sternotomy scar The mid-sternotomy scar suggests previous open heart surgery for repair of intracardiac defects (e.g. patch repair of ventricular septal defect, repair of tetralogy of Fallot), and valvar abnormalities (e.g. surgical aortic valvoplasty).
Lateral thoracotomy scar This scar can signify previous systemic-pulmonary arterial shunt insertion for duct-dependent cyanotic heart disease (e.g. pulmonary atresia with ventricular septal defect) or repair of coarctation of the aorta.
Praecordial impulses and thrills Knowledge of the topographic anatomy of the cardiovascular structures is important for the interpretation of the praecordial palpation findings. In the normal heart, the left ventricle occupies the apex, the body of the right ventricle underlies the left lower sternal border at the fourth and fifth intercostal spaces, the main pulmonary artery is beneath the left second intercostal space, and the aortic root is convex to the right of the sternum in the second intercostal space. A thrill is a palpable cardiac murmur. The intensity of the murmur, if accompanied by a thrill, is at least of grade 4/6. Interpretation of cardiac murmurs is discussed separately.
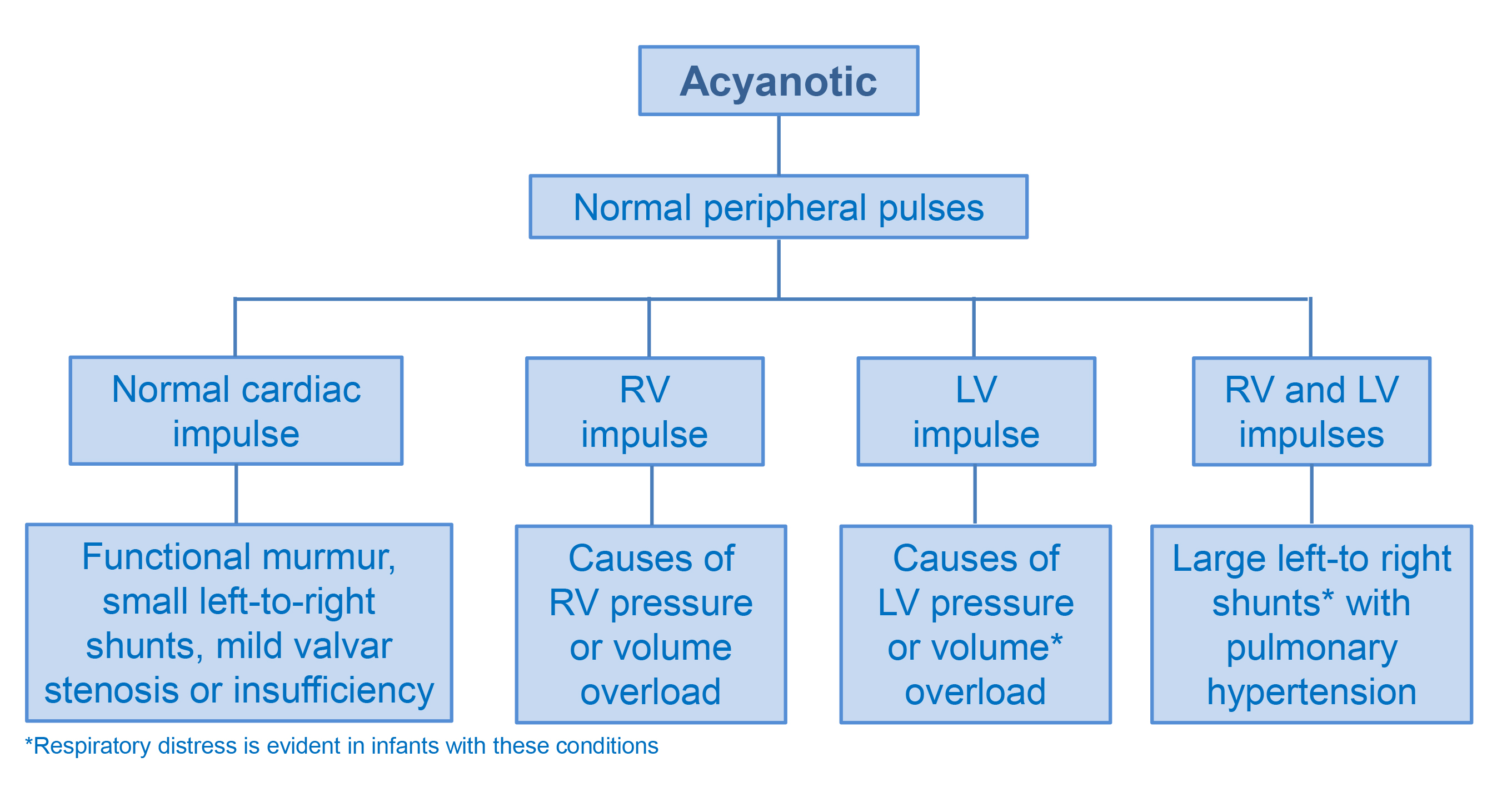
Cardiac apical pulsation Cardiac apical pulsation A strong apical cardiac impulse suggests either pressure loading or volume loading of the left ventricle. In pressure loading conditions of the left ventricle (e.g. aortic stenosis, coarctation of the aorta), the cardiac apex is usually not displaced laterally as the left ventricle is hypertrophic rather than dilated. On the other hand, in volume loading of the left ventricle (e.g. large left-to-right shunts, severe mitral or aortic regurgitation), the cardiac apex is displaced laterally.
Left parasternal impulse A strong left parasternal impulse suggests either pressure loading or volume loading of the right ventricle. Pressure loading conditions of the right ventricle can be caused by acyanotic (e.g. severe pulmonary valvar stenosis, pulmonary hypertension) or cyanotic (e.g. tetralogy of Fallot) conditions. On the other hand, volume loading of the right ventricle is usually caused by a large atrial septal defect.
Suprasternal pulsation Prominent suprasternal pulsation is related to pulsatile enlargement of either the main pulmonary trunk or ascending aorta. Underlying cardiac conditions to consider include aortic stenosis, pulmonary stenosis and less commonly, coarctation of aorta and persistent arterial duct.
The importance of holistic interpretation of the signs as described above cannot be overemphasized. Indeed, auscultation may not always be necessary to establish a diagnosis or a list of differential diagnosis. The following flowcharts illustrate this diagnostic approach as applied to asymptomatic children presenting with just a cardiac murmur, infants and children with symptoms of heart failure, and those with cyanosis.